Your eye test records are the medical foundation of your legal case. Without them, even a legitimate NAION claim becomes very difficult to prove. Here is exactly what you need, and why.
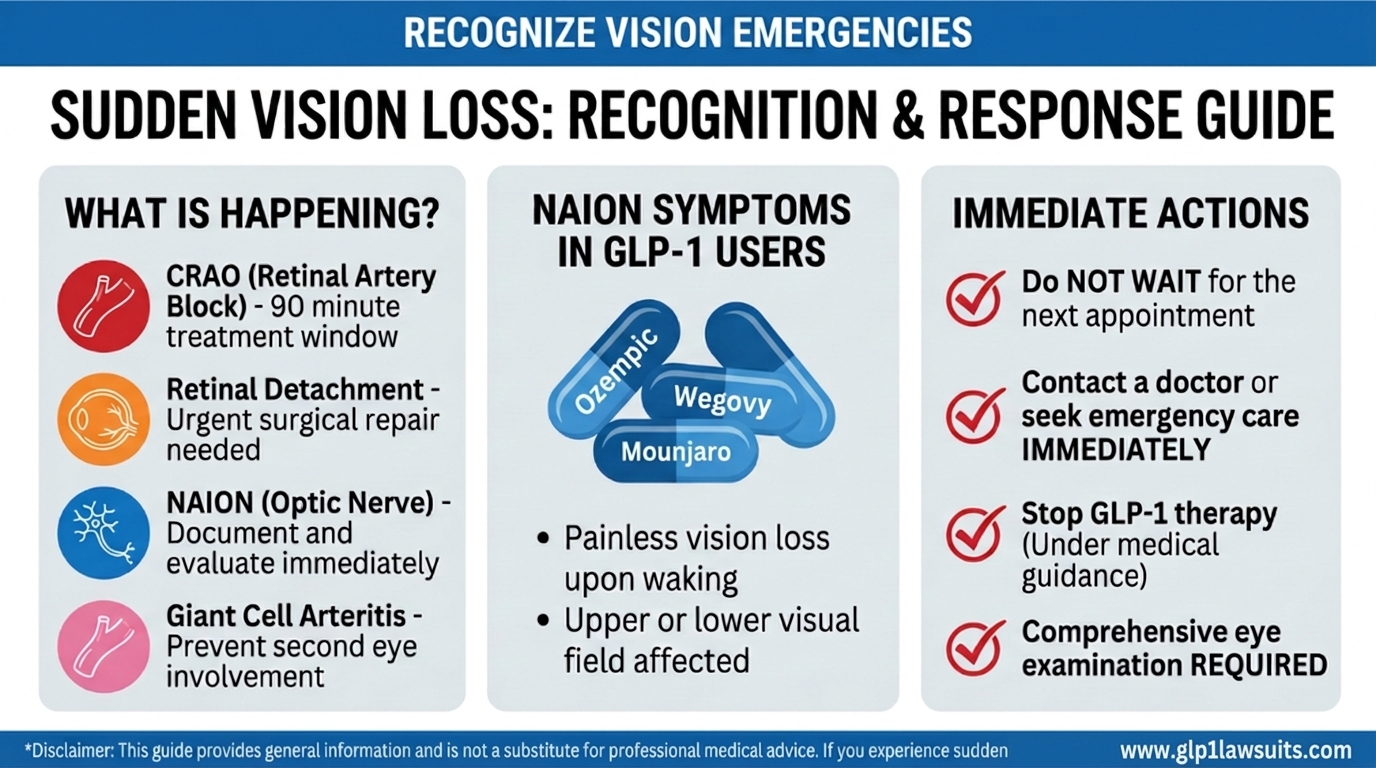
If you experienced sudden vision loss while taking a GLP-1 drug such as Ozempic, Wegovy, Mounjaro, or Zepbound and were diagnosed, or suspect you may have, non-arteritic anterior ischemic optic neuropathy (NAION), two things are simultaneously true: you need the right medical evaluation for your health, and you need thorough diagnostic documentation for your legal rights.
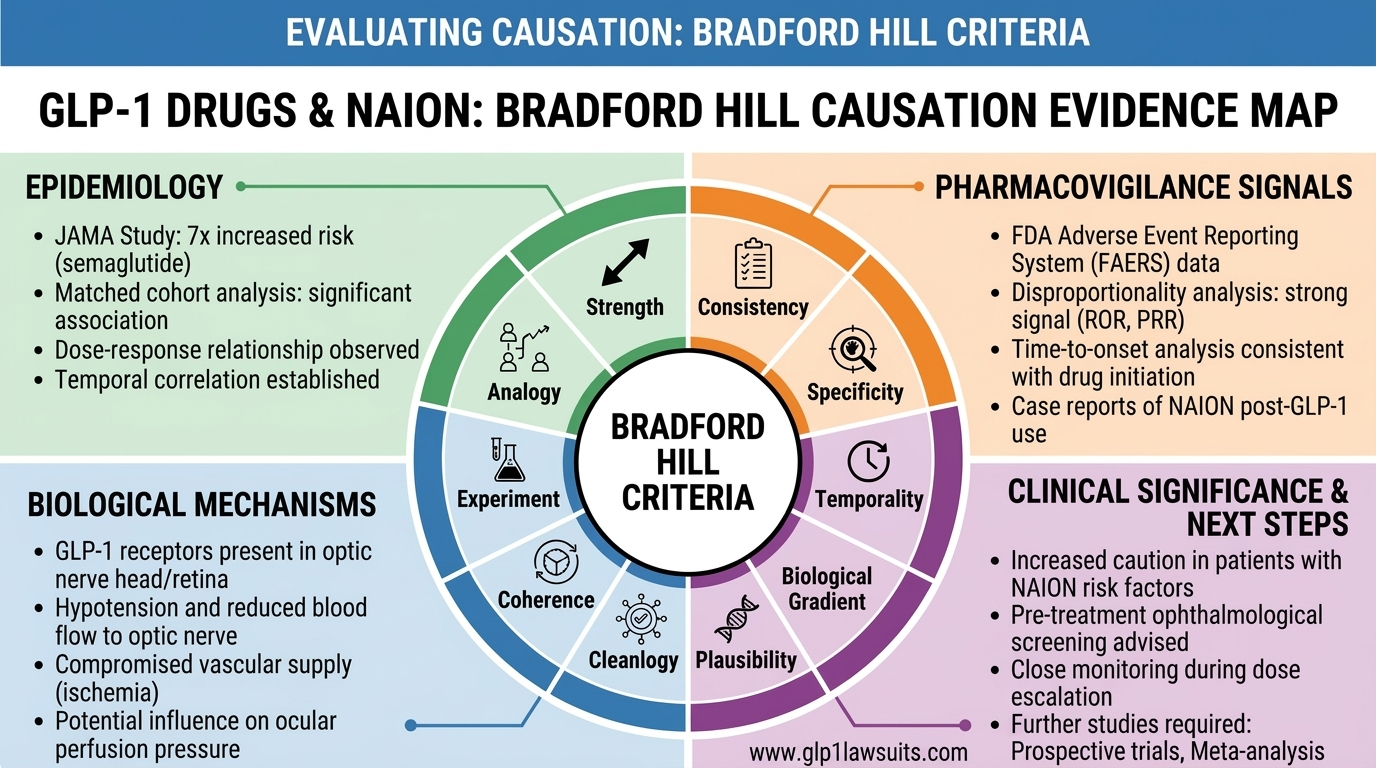
In pharmaceutical MDL litigation, the strength of your case depends heavily on the quality of your medical records. In the GI injury MDL (No. 3094), a court ruling requiring a formal gastric emptying study (GES) effectively eliminated many otherwise viable claims. In MDL 3163 (NAION), the equivalent battleground will be ophthalmologic documentation, whether plaintiffs have the objective eye test findings that can withstand Daubert scrutiny and support expert causation opinions.
This article explains every diagnostic test relevant to NAION, what each test is, what it shows, what normal and abnormal results look like, why it matters both medically and legally, and when in the course of NAION it should be performed.
Recommended Reading:
• What Is NAION? Understanding Non-Arteritic Anterior Ischemic Optic Neuropathy — Background on NAION and optic nerve damage
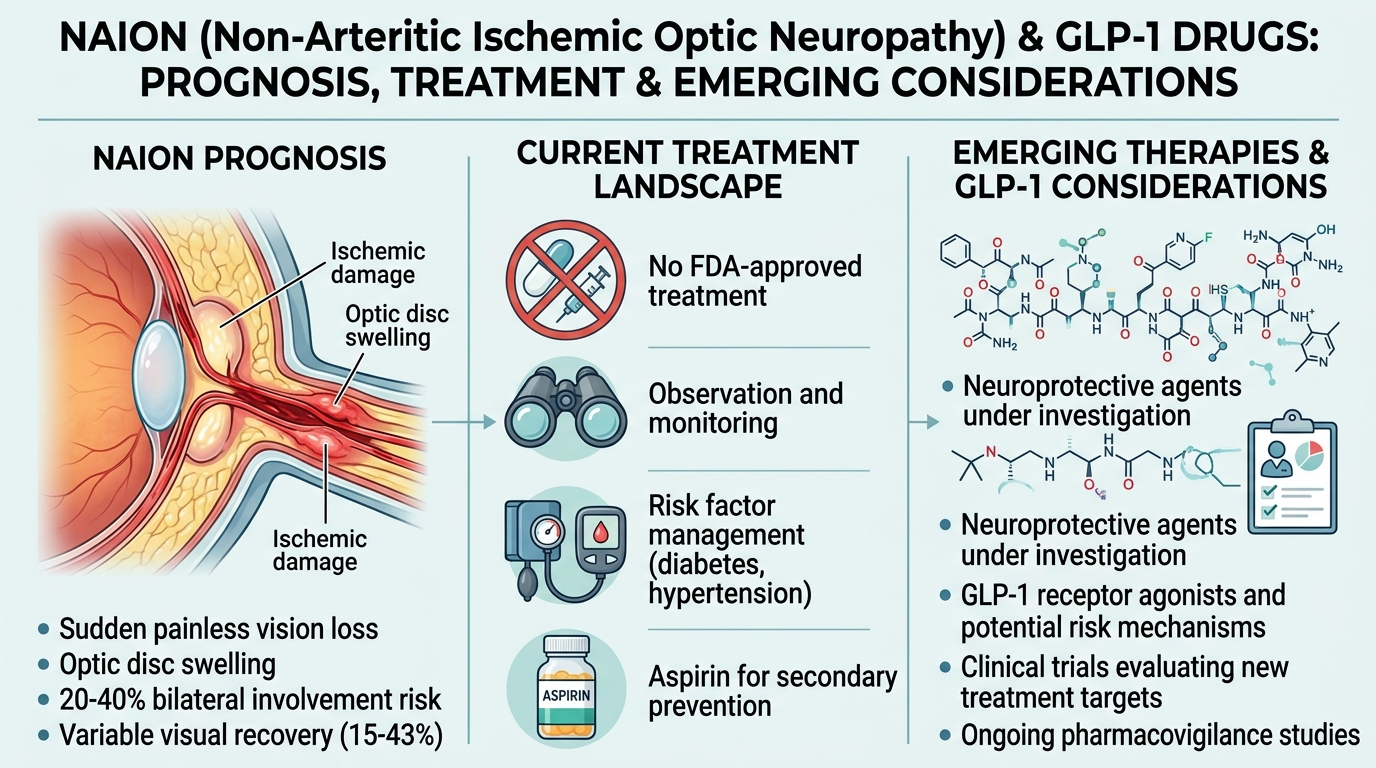
• Can NAION Be Reversed? Vision Loss Prognosis and Treatment — Prognosis and treatment information
• NAION MDL Update: GLP-1 Vision Loss Litigation Status — Latest NAION lawsuit MDL developments
---›
How NAION Is Diagnosed: The Clinical Framework
NAION is primarily a clinical diagnosis, meaning it is established through a combination of the patient’s history and a thorough ophthalmic examination, rather than by a single definitive laboratory test. The American Academy of Ophthalmology’s EyeWiki states clearly: in patients presenting with the typical history of acute, painless, unilateral vision loss with classic examination findings (hyperemic swollen optic disc, peripapillary hemorrhages, fellow eye with small cup-to-disc ratio), no additional testing is strictly required to make the diagnosis.
However, and this is critical for legal purposes, “not strictly required to diagnose” is not the same as “not required to document and prove.” In the context of a GLP-1 NAION lawsuit, objective, repeatable, quantitative test results are essential to:
- Establish the presence and severity of optic nerve damage beyond the subjective complaint of vision loss
- Exclude alternative diagnoses that defendants will argue caused the vision loss
- Document the permanent nature of injury over serial follow-up visits
- Quantify functional impairment for damages calculation
- Support expert causation opinions under the Rule 702 / Daubert standard
What follows is a test-by-test guide organized by category.
Category 1: Vision Function Tests
These tests measure how well the eye sees, both in terms of sharpness (acuity) and the full extent of the visual field. They form the functional baseline of any NAION workup.
1. Best-Corrected Visual Acuity (BCVA)
What it is: The standard Snellen eye chart test, performed with the patient’s best spectacle correction. Results are expressed as a fraction: 20/20 is normal; 20/200 means the patient can see at 20 feet what a person with normal vision sees at 200 feet.
What it shows in NAION: Visual acuity at the time of NAION onset ranges widely, from near-normal (20/15 to 20/30) to severely impaired (20/200 or worse). Approximately 50% of patients retain relatively good central acuity even with significant field loss because NAION often spares the central macula initially, while destroying peripheral and lower/upper field fibers.
Legal significance: Visual acuity is the most universally understood measure of vision. Serial BCVA measurements at presentation, 1 month, 3 months, 6 months, and 12 months document whether vision stabilized, partially recovered, or worsened, directly relevant to damages. A plaintiff who retains 20/60 vision but lost their lower visual field (altitudinal defect) cannot drive and may not be able to work, BCVA alone understates the functional loss and must be interpreted alongside visual field data.
Timing: Should be obtained at every ophthalmology visit from initial presentation through follow-up.
2. Visual Field Testing (Perimetry)
What it is: A test that maps the entire field of vision, central and peripheral, in each eye separately. The two main types used in clinical practice are:
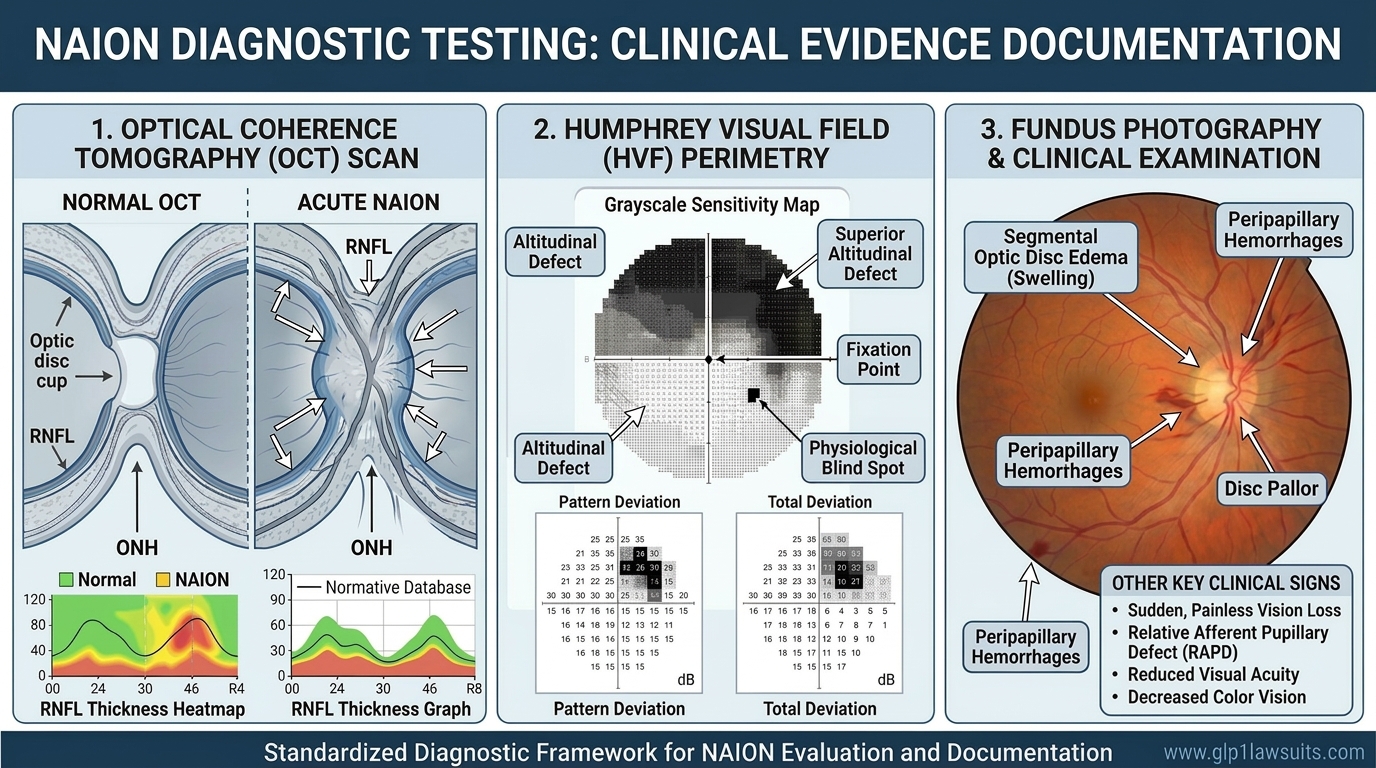
- Automated static perimetry (Humphrey Visual Field, HVF): The most widely used; the patient fixates on a central target while lights of varying intensity are flashed in different locations; the machine records which stimuli are detected. Standard protocols include the 24-2 (central 24-degree field) and 30-2 (central 30-degree field). Results are plotted as a grayscale map and expressed as mean deviation (MD) and pattern standard deviation (PSD).
- Goldmann kinetic perimetry: A manual test performed by a trained technician using a moving target; captures both the central field and the far periphery (beyond 30 degrees). Hayreh’s landmark NAION natural history study explicitly noted that automated perimetry misses important peripheral field loss in NAION and that Goldmann kinetic perimetry provides a more complete assessment of total visual disability.
What it shows in NAION: The hallmark visual field defect of NAION is the inferior altitudinal defect, loss of the lower half of the visual field in the affected eye. This occurs because NAION preferentially damages the superior optic nerve fibers, which subserve the inferior visual field. Other patterns include:
- Superior altitudinal defect (loss of upper field)
- Arcuate defects (curved loss tracking the nerve fiber bundles)
- Central or paracentral scotomas (focal blind spots)
- Diffuse depression (generalized loss of sensitivity across the entire field)
- Combined patterns
Legal significance: Visual field testing is arguably the most important functional test in a NAION legal claim because:
- It documents the pattern of field loss that is characteristic of NAION and distinguishable from glaucoma, retinal disease, and cortical causes
- Altitudinal field defects are the most legally compelling finding: they directly demonstrate inability to drive safely, read comfortably, navigate stairs, or perform many occupational tasks
- Serial field testing documents whether loss is permanent, progressive, or partially recovering — critical to both damages and countering defense arguments of temporary injury
- The printed HVF test result (grayscale map + numerical values + reliability indices) is a court-ready exhibit
Timing: Should be performed at initial presentation and repeated at 1–3 months, 6 months, and 12 months minimum. In chronic phase, annual testing monitors stability. Both the 24-2 or 30-2 automated test and a Goldmann test (where available) provide the most complete picture.
Legal warning: Patients who did not undergo visual field testing at the time of their vision loss, and whose symptoms are now chronic, should still undergo testing immediately. Chronic NAION produces stable, permanent field defects that remain documentable years after the acute event.
3. Color Vision Testing
What it is: Testing of the ability to discriminate colors, typically using Ishihara pseudoisochromatic plates or the Farnsworth-Munsell 100 Hue test. Results are expressed as number of errors or plates missed.
What it shows in NAION: Optic nerve disease, including NAION, causes acquired dyschromatopsia (loss or dulling of color vision), particularly affecting red-green discrimination, in the affected eye. Color vision loss may be present even when central acuity is relatively preserved.
Legal significance: Color vision testing provides additional objective evidence of optic nerve dysfunction, is easy to document, and is understandable to a lay jury. It also helps distinguish NAION from purely retinal causes of vision loss, where color vision may be relatively preserved.
4. Contrast Sensitivity Testing
What it is: Testing the ability to distinguish objects from their backgrounds, the “visual noise” threshold that standard acuity tests don’t capture. Performed with charts like the Pelli-Robson or CSV-1000.
What it shows in NAION: Many NAION patients have reduced contrast sensitivity even when Snellen acuity appears acceptable, reflecting the quality-of-vision impairment beyond simple letter recognition.
Legal significance: Contrast sensitivity deficits help explain why patients with seemingly “good” 20/40 acuity may still be unable to drive safely, read in low light, or perform visual tasks at work. This test is valuable in damages arguments where acuity alone might understate the functional impact.
Category 2: Pupillary Testing
5. Relative Afferent Pupillary Defect (RAPD): The Swinging Flashlight Test
What it is: A clinical examination finding, not a separate machine test. The examiner alternates a bright light between the two eyes (“swinging flashlight test”) and observes whether the pupils constrict equally. In a normal result, both pupils constrict the same amount regardless of which eye is illuminated. A relative afferent pupillary defect (RAPD), sometimes called a “Marcus Gunn pupil,” is present when the affected eye’s pupil constricts less in response to direct light than it does when light is shown in the other eye.
What it shows in NAION: RAPD is present in virtually all cases of unilateral NAION because the damaged optic nerve transmits a weaker afferent signal to the brain’s pupillary reflex centers. It is one of the most reliable objective signs of optic nerve damage and is difficult to fake or confound.
Legal significance: RAPD is a bedside finding that appears in every ophthalmology exam note from the time of initial presentation. It is often one of the first documented pieces of objective evidence in a NAION case. Its presence in initial records, made before any litigation, is powerful evidence that optic nerve damage was real, clinically apparent, and occurred when it was claimed.
Quantification: Newer technology (such as pupillography devices) can quantify RAPD numerically, which may be valuable for expert testimony and serial monitoring.
Category 3: Optic Nerve Imaging
These are the tests that most directly document structural damage to the optic nerve, and generate the objective, reproducible, court-ready imaging that makes NAION cases much stronger than symptom-based diagnoses.
6. Optical Coherence Tomography (OCT): The Single Most Important Test
What it is: OCT uses near-infrared light interferometry to generate high-resolution, cross-sectional images of the retina and optic nerve with micron-level precision. No radiation, no dye, no discomfort. For NAION, the two most relevant OCT measurements are:
- Peripapillary Retinal Nerve Fiber Layer (pRNFL) thickness: A circular scan around the optic disc measuring the thickness of the nerve fiber layer in each clock-hour quadrant. Reported as a global average and by sector (superior, inferior, nasal, temporal), with comparison to age-matched normative databases
- Ganglion Cell Layer + Inner Plexiform Layer (GCL+IPL) thickness: A macular scan measuring the thickness of the retinal ganglion cell body layer — the cells whose axons form the optic nerve
What it shows in NAION - Acute Phase (0–6 weeks):
- Optic disc edema: The pRNFL appears thickened due to swelling, the OCT hallmark of the acute phase
- GCL+IPL thinning: Crucially, research shows that GCL+IPL thinning is detectable within 1–2 months of NAION onset, appearing earlier than RNFL thinning, which is masked by the edema in the acute phase. GCL+IPL loss at 1–2 months showed moderate to strong correlation with visual acuity and mean visual field deviation
What it shows in NAION - Chronic Phase (3+ months):
- RNFL thinning: By 3–6 months, as edema resolves, RNFL thinning becomes the dominant finding. Published studies show mean global RNFL thickness of approximately 59.8 μm in NAION eyes vs. 95.1 μm in unaffected fellow eyes, a highly significant reduction representing irreversible nerve fiber loss
- Stability: Long-term studies confirm that RNFL thickness in NAION eyes stabilizes at approximately 6 months post-onset and remains stable thereafter, with no further significant loss on repeat scans, establishing the permanent, non-progressive nature of the injury
Legal significance: OCT is the gold standard structural documentation for NAION legal claims because:
- It generates quantitative, printed reports comparing the patient's nerve fiber layer to normative databases, the "red zone" printout showing values below normal limits is compelling visual evidence
- Serial OCT scans document the transition from acute edema to chronic atrophy, tracing the temporal arc of injury
- The 6-month stabilization finding means that a single OCT scan at 6+ months post-event can establish permanent structural loss with high confidence
- OCT images and reports are court-ready exhibits that a jury can understand: "this shows how much nerve tissue was permanently destroyed"
- Unlike subjective symptom reports, OCT findings cannot be fabricated and are consistent across multiple examinations
Timing:
- Acute phase: OCT at initial presentation documents edema and provides baseline GCL+IPL measurement
- 1–2 months: GCL+IPL thinning confirms early permanent neuronal injury even before RNFL changes
- 3–6 months: RNFL thinning quantifies permanent structural loss
- 12 months and annually thereafter: Confirms stability and documents no further progressive loss
OCT-Angiography (OCTA): An advanced variant that maps blood flow in the optic nerve head and retinal vasculature without dye injection. Studies suggest OCTA shows reduced flow in the optic disc perfusion in NAION, potentially tracking the vascular mechanism. While not yet standard of care for NAION diagnosis, OCTA findings are increasingly cited in research and may become relevant to causation arguments as the litigation develops.
7. Fundus Examination and Fundus Photography
What it is: Direct examination of the retina and optic nerve through a dilated pupil, using a slit lamp with fundus lens or indirect ophthalmoscope. Fundus photography captures a permanent photographic record of the optic disc and retina.
What it shows in NAION:
Acute phase:
- Hyperemic (pink/red), swollen optic disc: sectoral or diffuse swelling; a hyperemic appearance distinguishes NAION from arteritic AAION, where the disc typically appears pale and chalky white
- Peripapillary splinter/flame-shaped hemorrhages: small bleeds at the disc margin, present in the majority of acute NAION cases
- Swollen disc with minimal cupping: in contrast to glaucoma, where cupping is prominent
- Fellow eye with small cup-to-disc ratio: the "disc-at-risk" finding, present in over 90% of NAION patients
Chronic phase (weeks to months later):
- Optic disc pallor: the swollen disc fades to a pale, atrophic appearance, indicating permanent nerve fiber loss
- Pallor pattern matches the pattern of visual field loss, e.g., superior disc pallor corresponding to inferior altitudinal field defect
Legal significance: Fundus photographs taken at the time of initial presentation are irreplaceable, they document the acute optic disc swelling that proves the event occurred and when it occurred. Photographs taken weeks to months later documenting pallor establish permanence. These images are highly persuasive courtroom exhibits.
Practical note: Ask your ophthalmologist explicitly whether fundus photographs were taken at each visit. Many practices take them routinely; some do not. If photographs were not taken during the acute phase, this is a gap in your medical record that may need to be addressed through contemporaneous exam notes and OCT.
8. Fluorescein Angiography (FA)
What it is: A test in which fluorescent dye (sodium fluorescein) is injected intravenously and photographs are taken as the dye circulates through the retinal and choroidal blood vessels. The pattern of dye filling and leakage reveals vascular function in detail.
What it shows in NAION: In the acute phase, FA classically demonstrates delayed filling of the optic disc, the posterior ciliary arteries supplying the optic nerve head fill more slowly than normal, consistent with the ischemic mechanism. FA also shows late leakage from the swollen optic disc as the blood-optic nerve barrier is disrupted.
What FA rules out: In giant cell arteritis (AAION), FA shows choroidal non-perfusion, large areas of the choroid fail to fill at all, indicating widespread posterior ciliary artery occlusion. The absence of choroidal non-perfusion on FA is strong evidence supporting NAION rather than AAION, and rules out central retinal artery occlusion, retinal vein occlusion, and other vascular conditions.
Legal significance: FA provides direct imaging evidence of the vascular event, the actual delayed perfusion of the optic nerve head that caused the infarction. While not required in every case, FA findings can be powerful in Daubert challenges because they go to the specific causation question: did blood flow to the optic nerve actually decrease? FA also excludes alternative diagnoses, strengthening the NAION diagnosis against defense attempts to attribute the vision loss to other causes.
Category 4: Blood Tests: Ruling Out Arteritic Cause
9. Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP)
What they are: Blood tests measuring levels of systemic inflammation. ESR measures how quickly red blood cells settle in a tube; CRP is a direct inflammatory marker. Both are elevated in giant cell arteritis (GCA), the condition that causes arteritic anterior ischemic optic neuropathy (AAION), which is a medical emergency requiring immediate steroid treatment.
Why they are critical in NAION workup: Every patient presenting with acute vision loss and optic disc swelling must have same-day ESR and CRP testing to rule out GCA/AAION. A markedly elevated ESR (especially > 50–60 mm/hr) or CRP signals AAION, which requires emergency systemic corticosteroids to prevent complete vision loss and involvement of the fellow eye. Normal ESR and CRP strongly support NAION rather than AAION.
Important nuance: Normal ESR/CRP do not absolutely rule out GCA, approximately 4% of biopsy-proven GCA patients have normal inflammatory markers. When clinical suspicion for GCA is high despite normal labs (jaw claudication, scalp tenderness, age > 70, profound vision loss), temporal artery biopsy may still be warranted.
Legal significance: The presence of normal ESR and CRP in the initial workup documents that the treating physician appropriately evaluated and excluded the arteritic cause, supporting the NAION diagnosis and demonstrating that standard of care was followed. Defense experts may attempt to argue the diagnosis was incorrect; normal inflammatory markers are part of the differential diagnosis exclusion that makes NAION diagnosis robust.
10. Additional Blood Tests for Selected Patients
In patients with NAION who are younger than 50, bilateral at onset, or who have other atypical features, additional blood tests may be ordered to evaluate for hypercoagulable states and other systemic causes:
- Complete blood count (CBC): Rules out polycythemia (elevated red cell count) that increases blood viscosity
- Antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-β2 glycoprotein I): Rule out antiphospholipid syndrome, a thrombophilic condition associated with NAION in younger patients
- Protein C, Protein S, Factor V Leiden, prothrombin gene mutation: Inherited thrombophilias that can predispose to optic nerve ischemia
- Homocysteine levels: Elevated homocysteine is a vascular risk factor associated with NAION
- Fasting glucose and HbA1c: Documents diabetes as a risk factor and co-existing condition relevant to GLP-1 use
- Lipid panel: Hyperlipidemia as a vascular risk factor
- ANA, ANCA: Rules out systemic vasculitis or inflammatory optic neuropathy
Legal significance: In GLP-1 NAION cases, thorough workup for alternative causes is essential because defendants will argue that the patient’s NAION resulted from pre-existing conditions, diabetes, hypertension, hypercoagulability, rather than the drug. Negative alternative workup strengthens the causal link to GLP-1 therapy.
Category 5: Neuroimaging
11. MRI of the Brain and Orbits with Gadolinium Contrast
What it is: Magnetic resonance imaging of the brain and orbital structures, typically with and without intravenous gadolinium contrast, using dedicated orbital imaging sequences including high-resolution T2-weighted and contrast-enhanced T1-weighted imaging.
When MRI is indicated in NAION:
MRI is not required for every NAION patient when the clinical picture is typical. However, it is indicated when:
- Atypical features: Progressive vision loss beyond 2 months (NAION is typically acute-onset and then stable or slowly improving, progressive worsening suggests compressive or inflammatory disease)
- Bilateral simultaneous involvement at onset: Unusual for NAION; raises concern for inflammatory or compressive disease
- Young patient without vascular risk factors: NAION in a patient under 50 with no diabetes, hypertension, or sleep apnea demands investigation for optic neuritis, compressive lesion, or infiltrative disease
- Prolonged disc edema (beyond 8–10 weeks): May suggest optic neuritis or infiltrative optic neuropathy
- Pain with eye movement: Strongly suggests optic neuritis rather than NAION
- Recurrent episodes in the same eye: NAION does not typically recur in the same eye; recurrence suggests optic neuritis
What MRI shows in NAION vs. other conditions:
- NAION: Normal optic nerve or mild T2 signal change (hyperintensity) in the intra-orbital segment; no or minimal gadolinium enhancement of the optic nerve, a critical finding
- Optic neuritis: Almost always shows prominent gadolinium enhancement of the optic nerve on MRI, the absence of enhancement argues strongly for NAION over optic neuritis
- Compressive lesion: Mass or meningioma visible; optic nerve displacement
- Infiltrative disease: Abnormal nerve signal and enhancement pattern suggesting sarcoidosis, lymphoma, or other infiltration
- Demyelinating disease (MS): May show periventricular white matter lesions in addition to optic nerve changes
Legal significance: MRI serves a critical role in excluding alternative diagnoses, particularly optic neuritis, which shares some clinical features with NAION. Defense experts in MDL 3163 will argue that plaintiffs’ vision loss was caused by pre-existing conditions or alternative diagnoses rather than GLP-1 drugs. An MRI showing the absence of optic nerve enhancement (and the absence of compressive or inflammatory lesions) is objective evidence supporting the NAION diagnosis and closing the door on major differential diagnoses.
Advanced MRI: High-resolution 3D contrast-enhanced FLAIR (CE-FLAIR) imaging has emerged as a particularly useful sequence for distinguishing NAION from AAION, showing focal T2 hyperintensity without the extensive sheath involvement seen in arteritic cases, potentially valuable for complex diagnostic cases in the litigation.
12. Sleep Study (Polysomnography)
What it is: An overnight sleep study that measures brain waves, oxygen levels, heart rate, breathing patterns, and eye and leg movements during sleep. It is the gold standard for diagnosing obstructive sleep apnea (OSA).
Why it is relevant to NAION: OSA is one of the strongest independent risk factors for NAION and for fellow-eye involvement. Repeated nocturnal oxygen drops and blood-pressure swings in untreated OSA directly stress optic nerve perfusion. A sleep study is recommended in NAION patients with symptoms suggesting OSA, loud snoring, witnessed apneas, daytime sleepiness, and is standard StatPearls guidance.
Legal significance: Sleep apnea documentation has a dual role in litigation:
- If undiagnosed and untreated OSA is documented, it may represent a pre-existing, independent risk factor that defendants will attempt to use as an alternative causation argument
- Conversely, documenting that the treating physician and patient were unaware of OSA at the time of GLP-1 prescription and NAION onset, and that GLP-1 drugs added additional vascular stress, can support the specific causation narrative
Your NAION Documentation Checklist
If you believe your vision loss may be related to a GLP-1 drug, work with your attorney and eye care team to collect and preserve the following records:
Essential Records
- Ophthalmology visit notes from the time of initial vision loss, confirming acute NAION presentation
- Best-corrected visual acuity (BCVA) measurements, initial and follow-up
- Humphrey Visual Field (HVF) 24-2 or 30-2 printouts, showing altitudinal or other characteristic defects; serial exams ideal
- OCT reports with pRNFL and GCL+IPL data, acute phase (edema) and chronic phase (thinning); printed with normative comparison and sector data
- Fundus photographs of the affected and fellow eye, documenting disc swelling (acute) and pallor (chronic)
- RAPD documentation in exam notes, objective evidence of unilateral optic nerve dysfunction
- ESR and CRP lab results, normal values supporting NAION over arteritic AAION
Strongly Supportive Records
- Fluorescein angiography (FA) report and images, if performed, documents the ischemic mechanism
- MRI brain/orbit report, if performed, rules out optic neuritis and compressive lesions
- Sleep study results, documents OSA status
- Goldmann kinetic perimetry results, captures full peripheral field loss not shown on automated testing
Pharmacy and Prescriber Records
- Pharmacy fill history for all GLP-1 drugs, establishes which drug was taken, the dose, and duration of use
- Prescribing records from endocrinologist, primary care, or other prescriber, documents when the drug was started, dose escalation history, and any discussion of side effects
- Timeline linkage, records documenting when vision symptoms began relative to GLP-1 initiation or dose changes
What If You Don’t Have All These Tests?
Many patients did not receive a comprehensive NAION workup, particularly those whose vision loss was initially attributed to other causes, those who saw a general practitioner rather than an ophthalmologist, or those who recovered some vision and never sought full evaluation.
The good news: It is not too late in most cases. NAION leaves permanent structural evidence that can be documented even years after the acute event:
- Chronic RNFL thinning on OCT remains stable and measurable for years, a scan today can document permanent optic nerve loss from a NAION event in 2023
- Persistent visual field defects can be documented on perimetry at any time
- Optic disc pallor on fundus photography documents chronic post-NAION atrophy
- Fundus exam findings compatible with prior NAION can be documented in current ophthalmology notes with appropriate history
If you have not yet seen an ophthalmologist or neuro-ophthalmologist since your vision loss event, the most important first step, both medically and legally, is to schedule a comprehensive evaluation immediately. An experienced GLP-1 litigation attorney can also help coordinate with medical experts to ensure your records fully document the extent and permanence of your injury.
Q&A: NAION Eye Tests and Vision Loss Claims
Q1. What is the most important eye test for a NAION legal claim?
Optical coherence tomography (OCT) is the single most important imaging test because it generates objective, quantitative, reproducible evidence of permanent optic nerve fiber loss. Serial OCT showing the transition from acute edema to chronic RNFL thinning, with values significantly below normative ranges, is among the most powerful forms of structural evidence available in NAION litigation. Visual field testing is equally critical for documenting functional impairment.
Q2. Can my legal claim still proceed if I never had a formal NAION diagnosis?
Potentially yes, if objective evidence consistent with NAION can be documented. Some patients experienced sudden vision loss, had limited medical evaluation, and were not formally diagnosed with NAION. A neuro-ophthalmology evaluation today, documenting chronic RNFL thinning, persistent visual field defects, optic disc pallor, and a history consistent with NAION onset, may be sufficient to establish the diagnosis in retrospect. Only a licensed attorney can evaluate the viability of your specific claim.
Q3. Why does the NAION MDL care so much about eye test records?
Because of what happened in the GI MDL. In MDL 3094 (gastroparesis claims), a federal judge ruled that a formal gastric emptying study was required to support causation expert opinions, a ruling that knocked out many otherwise viable cases. In MDL 3163 (NAION), objective ophthalmologic testing, particularly OCT, visual field tests, and fundus findings, is the equivalent battleground. Plaintiffs with thorough, serial ophthalmologic documentation are in a much stronger position under Daubert scrutiny than those relying solely on subjective symptoms.
Q4. What is the difference between visual acuity testing and visual field testing?
Visual acuity measures how sharp and detailed central vision is (e.g., reading the Snellen eye chart). Visual field testing maps the full extent of vision, peripheral, upper, and lower, in each eye. In NAION, many patients retain relatively good central acuity but have devastating visual field loss (particularly the lower half of vision), which impairs driving, reading, and many occupational tasks. Both tests together provide a complete picture of NAION-related functional impairment.
Q5. What does it mean if I have a “relative afferent pupillary defect”?
A relative afferent pupillary defect (RAPD), detected with the swinging flashlight test, means your affected eye sends a weaker signal through the optic nerve to the brain’s pupillary reflex centers. It is an objective, reliable sign of optic nerve damage present in virtually all cases of unilateral NAION. Its documentation in your ophthalmology records at the time of initial presentation is important evidence that optic nerve damage was real and clinically apparent.
Q6. How many ophthalmology visits do I need to support my claim?
At a minimum, documentation from the time of initial vision loss plus at least one follow-up visit at 6–12 months (documenting chronic RNFL thinning and stable field defects) establishes the acute event and its permanent aftermath. Ideally, serial records at presentation, 1–3 months, 6 months, and 12 months provide the strongest longitudinal evidence of permanent injury. If you have only limited records, an experienced neuro-ophthalmologist can perform a comprehensive current evaluation and document findings consistent with prior NAION.
Q7. Should I see a general ophthalmologist or a neuro-ophthalmologist?
For both medical care and legal documentation, a neuro-ophthalmologist provides the most authoritative evaluation. Neuro-ophthalmologists specialize in optic nerve and visual pathway disorders, are experienced in the NAION diagnostic workup, and can provide the detailed, comprehensive exam records and expert opinions most valuable in litigation. If a neuro-ophthalmologist is not available, a general ophthalmologist or retina specialist can perform most of the required testing, but a neuro-ophthalmology consultation should be sought for any complex or disputed case.
Why Work With Us
Exclusive Focus on GLP‑1 Injuries
Our practice is dedicated entirely to GLP-1 medication injuries, including NAION vision loss, gastroparesis, ileus, and related complications. This is not a side project; it is the core of what we do every day.
- Deep, case-specific knowledge of Ozempic, Wegovy, Mounjaro, Zepbound, and related medications
- Familiarity with NAION ophthalmologic diagnostics and how each test supports causation and damages
- Hands-on experience with MDL procedures, Plaintiff Fact Sheet requirements, and case-management orders in complex pharmaceutical litigation
Because we live in this space, we know which test results are essential, which gaps in your records can be filled, and how to build the strongest possible evidentiary foundation for your NAION claim.
Integrated Medical Expert Network
NAION cases require medical experts who understand ophthalmology as much as law. We work with:
- Neuro-ophthalmologists and ophthalmologists who can review your records, perform current evaluations, and provide expert opinions on diagnosis and causation
- Pharmacologists who can explain GLP-1 mechanisms and their effects on optic nerve perfusion
- Life-care planners who quantify future ophthalmology monitoring, low vision rehabilitation, and assistive technology needs
- Vocational experts who document how vision loss has affected your ability to work
Proven Results in Complex Drug Litigation
Our attorneys have recovered millions of dollars for clients in pharmaceutical MDLs and complex injury cases. We understand the Daubert landscape, the bellwether process, and how to negotiate maximum recovery against large pharmaceutical defendants.
No Upfront Costs - Ever
We work on a contingency-fee basis, which means no attorney fee unless we win, we advance all litigation costs, and your initial consultation is completely free. You risk nothing by finding out whether you have a case.
Comprehensive Case Management
We handle every aspect of building your evidentiary record:
- Obtaining all ophthalmology, pharmacy, and prescriber records
- Coordinating current neuro-ophthalmology evaluations where records are incomplete
- Preparing and submitting Plaintiff Fact Sheets and MDL documentation
- Working with medical experts to ensure your records support the strongest possible causation opinion
- Keeping you informed at every step and pursuing maximum compensation
Contact Us for a Free Consultation
Your eye records are the key to your case, and time is running out to gather them.
If you took Ozempic, Wegovy, Mounjaro, or Zepbound and experienced sudden vision changes or were diagnosed with NAION, your legal rights may be worth pursuing in MDL 3163. The statute of limitations is running. Don’t wait.
Visit www.GLP1Lawsuits.com to:
- Get a free case evaluation
- Speak with an experienced pharmaceutical-litigation attorney about your NAION records and legal options
- Learn more about MDL 3163 and what to expect from the claims process
- Get a timeline-specific analysis of your GLP-1 use, diagnosis, and documentation
- Join others seeking justice for preventable, permanent vision loss
No upfront fees. No costs unless we win your case.
Sources Cited
| # | Authority | Description |
|---|---|---|
| 1 | AAO EyeWiki - NAION | Clinical diagnosis criteria, required workup, and when additional testing is indicated. Updated November 2024 |
| 2 | NIH / StatPearls - NCBI Bookshelf | Kaur K, Margolin E. “Nonarteritic Anterior Ischemic Optic Neuropathy.” StatPearls. September 2025 - comprehensive clinical workup including neuroimaging and polysomnography indications |
| 3 | Brigham and Women’s Hospital - Neuro-Ophthalmology | Patient-facing clinical overview of NAION diagnosis workup: history, acuity, color vision, peripheral visual field, blood work, optic disc evaluation |
| 4 | Hayreh SS - NAION Natural History Study, PMC2782939 | Visual field assessment in NAION: importance of Goldmann kinetic perimetry for peripheral field; visual acuity vs. visual field disability |
| 5 | IOVS - GCL+IPL thinning in NAION (Levin et al.) | Retinal ganglion cell layer thinning within 1–2 months of NAION: GCL+IPL is an earlier biomarker than RNFL in acute NAION; correlation with acuity and mean deviation |
| 6 | PMC - Long-term RNFL changes in NAION (PMC3632631) | Mean global RNFL 59.8 μm in NAION vs. 95.1 μm in fellow eyes at 6 months; stability at 13 months; quantifying permanent structural loss |
| 7 | PMC - Retinal layer changes over time in NAION (PMC8169768) | Peripapillary RNFL thinning and macular ganglion cell loss in chronic NAION on OCT |
| 8 | PMC - High-resolution MRI in NAION (PMC12635806) | HR 3D CE-FLAIR MRI features in NAION: focal T2 hyperintensity, minimal enhancement; distinguishing NAION from AAION on MRI. December 2025 |
| 9 | MRI differentiation of ON vs. NAION (ScienceDirect) | Absence of gadolinium enhancement on MRI is key distinguishing feature of NAION vs. optic neuritis |
| 10 | PMC - Normal ESR/CRP in GCA (PMC8900556) | ~4% of biopsy-proven GCA patients have normal inflammatory markers; ESR/CRP interpretation in NAION workup |
| 11 | EyeWiki - Giant Cell Arteritis | Combined ESR/CRP sensitivity 99% for GCA diagnosis; emergency differentiation from NAION |
| 12 | AAO EyeWiki - GCA | Emergency temporal artery biopsy and immediate corticosteroid treatment for AAION; differential from NAION |
| 13 | Glaucoma Today - NAION: What to Do and When | Acute phase fundus findings: hyperemic disc swelling, peripapillary hemorrhages; visual field altitudinal defects |
| 14 | Injuries and Accidents: Ozempic Vision Loss Claims | Key ophthalmologic records supporting NAION claims: diagnosis, imaging, medical documentation. March 2026 |
| 15 | JPML Transfer Order - MDL No. 3163 | Separate NAION MDL creation; distinct medical/scientific issues; common questions re: labeling and warning decisions. December 2025 |
| 16 | E.D. Pa. - MDL 3094 Rule 702 / Daubert Order | GES requirement for GI causation experts, context and cautionary precedent for NAION documentation requirements. August–September 2025 |
Disclaimer
This article provides general medical and legal information about NAION diagnostic testing and GLP-1 litigation and does not constitute medical or legal advice. For diagnosis, testing, and treatment of vision problems, consult a qualified ophthalmologist or neuro-ophthalmologist. For guidance on your specific legal situation, including what records you have, whether they are sufficient for a claim, and the applicable statute of limitations, consult a licensed pharmaceutical litigation attorney. Each case is unique and past results do not guarantee future outcomes.
© 2026 GLP1lawsuits.com | All Rights Reserved
Last reviewed by an attorney: March 2026