If you are experiencing sudden vision loss right now - stop reading and call 911 or go to an emergency room immediately. Every minute matters.
Sudden vision loss is one of the most frightening and medically serious symptoms a person can experience. It can signal a stroke, a retinal artery occlusion (an “eye stroke”), a detached retina, giant cell arteritis, or, increasingly in the age of GLP-1 drugs like Ozempic, Wegovy, Mounjaro, and Zepbound, a condition called non-arteritic anterior ischemic optic neuropathy (NAION).
Some of these conditions have treatment windows measured in minutes to hours before damage becomes permanent. Others, like NAION, have no reversible window at all, but still demand urgent evaluation to confirm the diagnosis, protect the unaffected eye, and preserve the medical documentation that may be critical for a legal claim later.
This article tells you exactly what to do, when to do it, and why, with the clinical detail you need to make the right decision in a frightening moment.
For a full explanation of NAION and how GLP-1 drugs are linked to it, read: Understanding the Growing Concerns Around GLP-1 Drugs and Vision Loss (NAION) For the NAION diagnostic workup and what tests you’ll need, read: NAION Eye Tests Required for Vision Loss Claims For NAION prognosis and treatment options, read: Can NAION Be Reversed? Vision Loss Prognosis and Treatment
The Golden Rule: All Sudden Vision Loss Is an Emergency
Before anything else, understand this foundational principle shared by every major ophthalmology and emergency medicine organization:
There is no such thing as sudden vision loss that is safe to “wait and see.”
More than 7 million Americans experience sudden vision loss annually, and the causes range from immediately life-threatening (stroke) to permanently disabling (NAION, retinal artery occlusion) to surgically reversible if caught in time (retinal detachment). No patient, no matter how mild the symptoms seem, can reliably self-diagnose which category their vision loss falls into without a trained clinician and diagnostic equipment.
The most dangerous thing you can do when vision suddenly changes is decide it will probably pass on its own.
Emergency vs. Urgent: How to Decide in the Moment
Not every vision problem requires calling 911, but sudden vision loss almost always does. Here is the decision framework:
CALL 911 OR GO TO THE EMERGENCY ROOM IMMEDIATELY IF YOU HAVE:
- Complete or near-complete vision loss in one or both eyes, any rapid, dramatic decrease in vision
- A curtain, shadow, or dark veil descending across part of your vision
- Loss of the top or bottom half of your visual field (altitudinal defect, the classic NAION presentation)
- Sudden vision loss upon waking, you went to sleep with normal vision and woke up unable to see clearly in one eye (the hallmark NAION pattern)
- Transient vision loss that has already resolved, “it came back, so I’m fine” is one of the most dangerous assumptions in medicine; transient vision loss may signal an impending stroke (see amaurosis fugax, below)
- Sudden vision loss accompanied by headache, jaw pain, scalp tenderness, or temple pain, these are classic signs of giant cell arteritis (temporal arteritis), a true medical emergency that can cause permanent bilateral blindness within hours
- Sudden vision loss with facial drooping, arm weakness, slurred speech, or confusion, this is a stroke; call 911 immediately
- A sudden shower of new floaters with or without flashes of light, classic warning signs of a retinal tear or detachment
- A dark area spreading across vision from one side, may indicate retinal detachment or vitreous hemorrhage
- Severe eye pain with vision loss, halos around lights, nausea, or vomiting, possible acute angle-closure glaucoma, a true emergency; intraocular pressure can destroy the optic nerve within hours
- Double vision that begins suddenly, may indicate a neurological emergency including aneurysm or brainstem stroke
SAME-DAY URGENT EYE CARE (Call your ophthalmologist first; go to ER if unavailable):
- New onset of a few floaters without flashes and without vision loss, warrants same-day evaluation but not necessarily 911
- Temporary blurring that fully resolves, still needs urgent evaluation the same day, especially in GLP-1 users
- Mild, gradual blurring over hours without other symptoms, urgent but not necessarily an ER
IF IN DOUBT: GO TO THE ER
Emergency departments can provide initial stabilization, blood pressure and stroke workup, and emergency ophthalmology consultation. It is always better to go and be reassured than to wait at home while a treatable condition progresses beyond the window for intervention.
Why Time Is Everything: The Emergency Vision Loss Clock
Different causes of sudden vision loss have radically different, and unforgiving, treatment windows. This is why the moment you notice vision loss is not the time to search the internet. It is the time to act.
Central Retinal Artery Occlusion (CRAO): Minutes to Hours
CRAO, often called an “eye stroke,” occurs when the central artery supplying the retina becomes blocked, cutting off oxygen to the light-sensitive cells that send visual signals to the brain. It is among the most time-critical emergencies in ophthalmology.
- Clinical time window: Retinal ganglion cells, the neurons that transmit vision, begin to undergo irreversible infarction after as little as 12–15 minutes of complete ischemia, though clinically significant visual recovery may still be possible with treatment within 4–6 hours of onset for incomplete occlusions
- 240-minute threshold: Beyond 240 minutes of complete CRAO, massive irreversible ischemia of the retina is expected, comparable to the 4.5-hour thrombolysis window in brain stroke
- Treatment: IV tissue plasminogen activator (tPA), ocular massage, anterior chamber paracentesis, hyperbaric oxygen, and other approaches, all require emergency-level intervention and carry the best chance of success the sooner they are initiated
- Stroke connection: CRAO shares the same thromboembolic mechanism as ischemic stroke, up to 25% of CRAO patients have an associated brain infarction, and patients with CRAO have a significantly elevated near-term stroke risk; full stroke workup is mandatory
CRAO vs. NAION: Both present as sudden, painless, unilateral vision loss. The critical distinction, made on fundus examination, is that CRAO shows retinal pallor and a classic cherry-red spot at the macula, while NAION shows an edematous, hyperemic optic disc without retinal pallor. You cannot reliably tell them apart without a dilated eye exam.
Giant Cell Arteritis (GCA / Temporal Arteritis): Hours
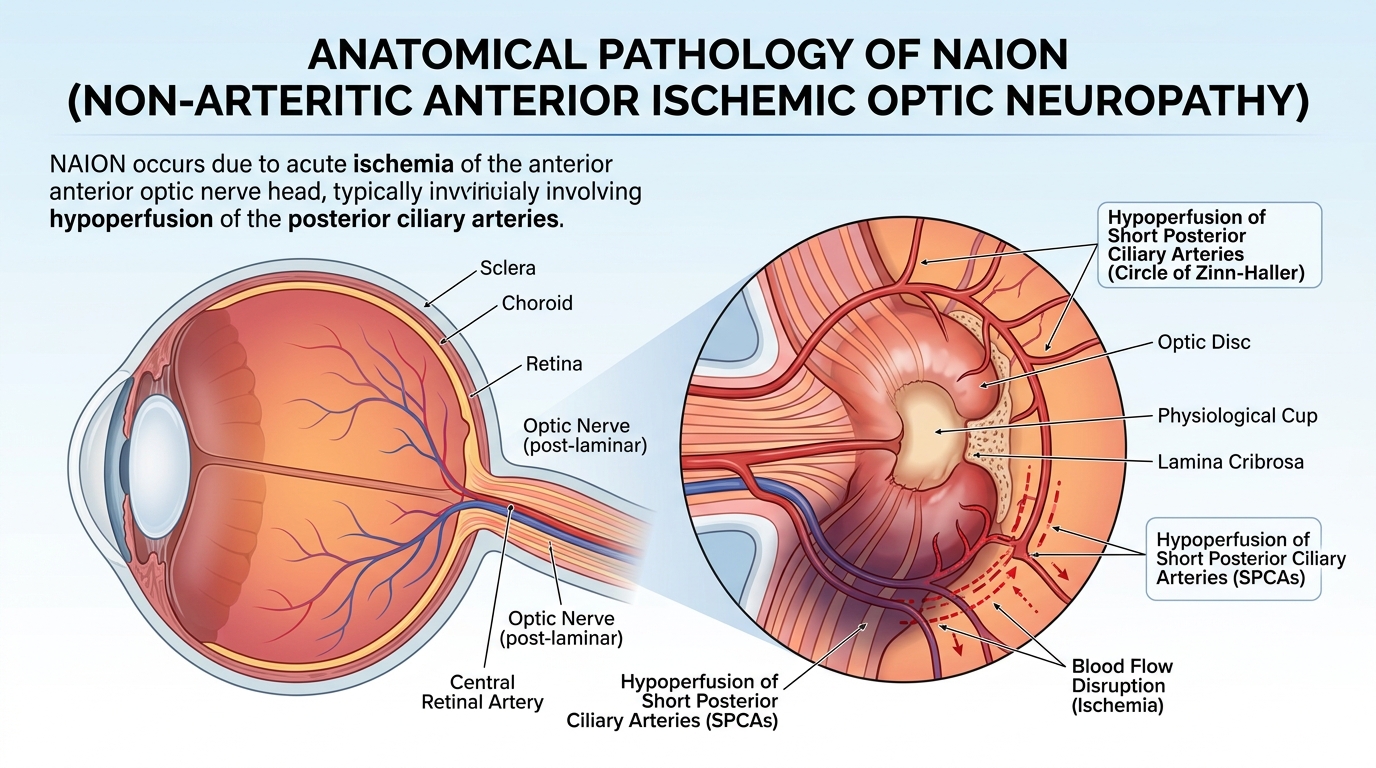
GCA is an inflammatory vasculitis of medium and large arteries, most commonly affecting the posterior ciliary arteries that supply the optic nerve. It is the cause of arteritic anterior ischemic optic neuropathy (AAION), a condition easily confused with NAION but far more aggressive and immediately treatable.
- Why it’s a true emergency: In GCA, once vision is lost in one eye, the fellow eye is at risk of losing vision within hours to days without immediate treatment. Approximately 25–50% of untreated GCA patients lose vision in the second eye shortly after the first
- Treatment window: High-dose systemic corticosteroids (oral prednisone 40–60 mg/day, or IV methylprednisolone 250 mg every 6 hours for patients with active vision loss) must be started immediately, ideally the same day, before even confirming the diagnosis with temporal artery biopsy. Mayo Clinic, Cleveland Clinic, and every major ophthalmology organization are emphatic: do not wait for biopsy results before starting steroids
- Who is at risk: Adults over 50 (average onset age 70+); women more than men; patients of Northern European ancestry; those with polymyalgia rheumatica
- Distinguishing symptoms from NAION: GCA vision loss may be accompanied by new headache (especially temporal), jaw claudication (pain when chewing), scalp tenderness (pain when combing hair), fatigue, fever, and weight loss, symptoms that NAION patients typically do not have. ESR and CRP are dramatically elevated in most GCA cases. The optic disc in AAION appears chalky white and pale (in contrast to the pink, hyperemic disc of NAION)
- If you are on a GLP-1 drug: GCA preferentially affects the same age group and vascular risk profile as many GLP-1 users. Any sudden vision loss in a patient over 60 who is on Ozempic, Wegovy, Mounjaro, or Zepbound must be evaluated for GCA immediately, the initial test and treatment decision cannot wait
Retinal Detachment: Hours to Days
Retinal detachment occurs when the neurosensory retina separates from the underlying retinal pigment epithelium, cutting off the photoreceptors from their blood supply. If the detachment involves the central macula (“macula-off”), permanent central vision loss occurs within hours.
- Warning symptoms: A sudden shower of new floaters, arcs of flashing light (photopsia), followed by a shadow, curtain, or veil spreading across vision from the periphery
- Macula-on vs. macula-off: If the macula is still attached, urgent same-day or next-day surgery typically preserves central vision. Once the macula detaches, even successful surgical reattachment may leave permanent visual impairment
- Treatment: Surgical reattachment, pneumatic retinopexy, scleral buckle, or vitrectomy, performed by a retina surgeon. No medical therapy reverses retinal detachment
- Key distinction from NAION: Retinal detachment almost always has prodromal floaters and flashes before the “curtain,” NAION typically has none. Detachment symptoms progress over minutes to hours; NAION vision loss is often noticed suddenly upon waking
Acute Angle-Closure Glaucoma: Hours
Acute angle-closure glaucoma occurs when the iris blocks the drainage angle of the eye, causing a sudden, dramatic rise in intraocular pressure. Untreated, the elevated pressure destroys optic nerve fibers within hours.
- Symptoms: Severe eye or periorbital pain, blurred vision, halos around lights, headache, nausea, and vomiting, the pain and nausea component distinguishes this from NAION, which is painless
- Treatment window: Emergency eye drops (to lower pressure immediately), followed by laser iridotomy or surgery; delay of even a few hours can result in permanent optic nerve damage and chronic glaucoma
- Relation to GLP-1 users: Not directly linked to GLP-1 drugs, but important to distinguish from NAION in the acute presentation
Amaurosis Fugax (Transient Vision Loss): A Stroke Warning You Cannot Ignore
Amaurosis fugax is a temporary, painless loss of vision in one eye, typically described as a gray curtain descending and then lifting, lasting seconds to minutes, with complete spontaneous recovery. It is caused by a temporary blockage of blood flow to the retina, most commonly from a microembolus originating in the carotid artery or the heart.
Why it is an emergency even though vision returns:
Amaurosis fugax is a transient ischemic attack (TIA) of the eye, a warning that a full stroke may be imminent. Patients with untreated amaurosis fugax have an approximately 10–15% risk of stroke within the first year, with the highest risk in the days immediately following the episode. Early carotid imaging, cardiac workup, and antiplatelet or anticoagulant therapy can dramatically reduce this risk, but only if the patient presents immediately.
Never dismiss temporary vision loss as “fine because it came back.” Get emergency evaluation the same day it occurs, regardless of complete visual recovery.
Distinguishing from NAION: NAION does not typically resolve, vision loss is permanent from the time of onset. Amaurosis fugax resolves completely within minutes. If vision has fully returned, the presentation is almost certainly not NAION, but it is still an emergency for stroke workup.
Optic Neuritis: Urgent (Less Immediately Time-Critical, But Still Prompt)
Optic neuritis is inflammation of the optic nerve, most commonly associated with multiple sclerosis or other demyelinating conditions. It typically presents as vision loss developing over hours to days, often with pain with eye movement (which NAION does not cause), and affects younger patients (20s–40s).
- Treatment: IV methylprednisolone speeds recovery of visual acuity (though does not change final visual outcome) and may delay conversion to MS
- Key distinction from NAION: Eye pain on movement strongly suggests optic neuritis, not NAION. Patients with optic neuritis are typically younger, lack the vascular risk factor profile of NAION patients, and show gadolinium enhancement of the optic nerve on MRI
- Why this matters for GLP-1 users: If you are on Ozempic, Wegovy, Mounjaro, or Zepbound and develop painful vision loss, you still need urgent evaluation, but optic neuritis, not NAION, becomes the primary differential diagnosis
What NAION Vision Loss Feels Like: Knowing Your Specific Symptoms
Because NAION is now linked to GLP-1 drugs and is the focus of growing medical and legal attention, every GLP-1 user should know its specific symptom profile:
The Classic NAION Presentation
- Onset: Sudden, most patients notice the vision loss upon waking in the morning, having gone to sleep with normal vision. The ischemic event likely occurs during sleep when blood pressure is at its lowest (nocturnal hypotension)
- Pain: None - NAION is painless. Any significant eye pain with vision loss suggests a different diagnosis
- Laterality: One eye only, at least initially. Bilateral simultaneous onset is highly unusual for NAION
- Acuity: Variable, may range from very mild blurring to severe loss; approximately 50% of patients retain relatively normal central acuity while losing significant peripheral or altitudinal field
- The field defect: The most characteristic symptom is loss of the bottom half of vision (inferior altitudinal defect), patients often describe feeling as though they are looking through a darkened lower half of the visual field, or noticing they can no longer see the bottom portion of their phone screen, the floor, or the text at the bottom of a page
- Color vision: Colors may appear duller or washed out in the affected eye compared to the other
- Monocular testing: If you alternately cover each eye, you may notice a dramatic difference between what each eye sees; this is a key early clue
The One-Eye Cover Test - Do This Right Now
If you are a GLP-1 user concerned about your vision, medical experts recommend this simple self-test:
- Cover your right eye completely with your palm
- Look at a fixed object or text with only your left eye, note sharpness, completeness of field, color
- Switch, cover your left eye and look with only your right
- Compare the two experiences
If one eye sees significantly less clearly, less completely, or with duller color, especially if this is a change from normal, seek urgent ophthalmology evaluation that day.
The Morning Vision Check
Because NAION typically presents upon waking, ophthalmologists advise GLP-1 users with risk factors to briefly test each eye independently every morning upon waking, before getting up, simply cover each eye alternately and check that vision is symmetric and complete. This takes 10 seconds and could be the difference between documenting a fresh NAION event (with an acutely swollen optic disc, present only for 4–8 weeks) and missing the acute phase entirely.
When You Have Sudden Vision Loss on a GLP-1 Drug: Step by Step
If you are currently taking Ozempic, Wegovy, Mounjaro, Zepbound, Rybelsus, Trulicity, Saxenda, or any other GLP-1 receptor agonist and you experience sudden vision changes, here is exactly what to do:
Step 1: Act Immediately - Do Not Wait
Call 911, go to the nearest emergency room, or call your ophthalmologist’s emergency line. Do not drive yourself if vision is significantly impaired. Do not wait to see if vision improves. Do not search the internet first.
For any suspicion of stroke, GCA, retinal artery occlusion, or retinal detachment, conditions that may be confused with NAION, time is the most critical factor.
Step 2: Tell the Doctor You Are on a GLP-1 Drug
When you arrive at the ER or ophthalmology clinic, immediately and explicitly tell the treating clinician:
“I am currently taking [drug name and dose], a GLP-1 receptor agonist, and I have had sudden vision loss. I understand there is a potential link between GLP-1 drugs and a condition called NAION.”
Many emergency physicians and general practitioners may not yet be aware of the GLP-1/NAION connection. Bringing it to their attention ensures it is considered in the differential diagnosis and properly documented in your medical records.
Step 3: Request and Document the Full Workup
Ask specifically for:
- Dilated fundus examination (optic disc evaluation)
- Best-corrected visual acuity measurement
- Intraocular pressure check (rules out acute glaucoma)
- Relative afferent pupillary defect (RAPD) testing
- ESR and CRP blood tests (rules out giant cell arteritis / AAION)
- Fundus photography if available
- Referral to an ophthalmologist or neuro-ophthalmologist for same-day or next-day follow-up
Step 4: Get a Neuro-Ophthalmology Appointment Within Days
Even if the ER confirms NAION and not a stroke or retinal detachment, the initial ER evaluation rarely includes the full diagnostic workup needed to establish your case medically and legally. Within 3–5 days, you should see a neuro-ophthalmologist for:
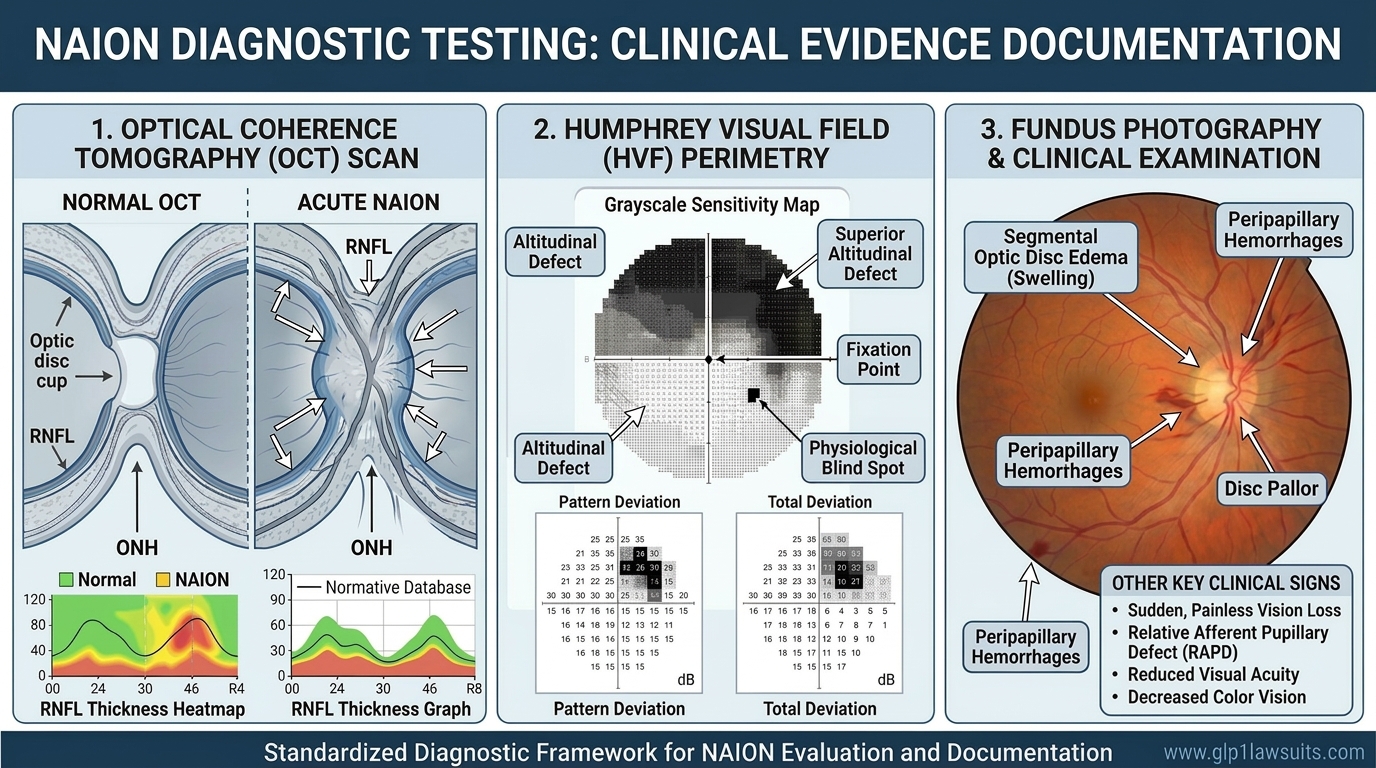
- Formal visual field testing (Humphrey 24-2 or 30-2, and ideally Goldmann kinetic perimetry)
- Optical coherence tomography (OCT) of the retinal nerve fiber layer and ganglion cell layer
- Complete ophthalmic examination and fundus photography
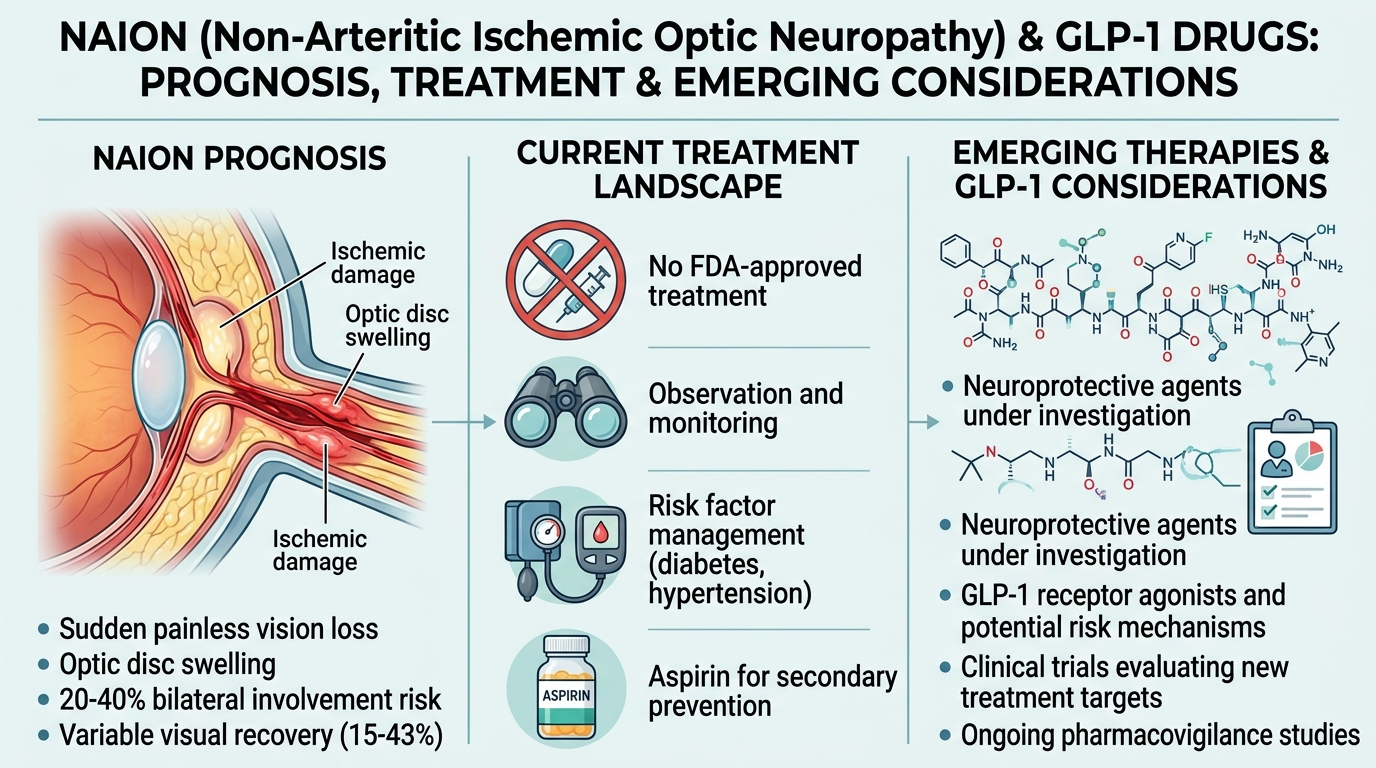
- Discussion of GLP-1 medication discontinuation per EMA/WHO guidance for confirmed NAION
Step 5: Do Not Stop the GLP-1 Drug Without Medical Guidance
While European and WHO guidance recommends discontinuing semaglutide if NAION is confirmed, you should not abruptly stop any medication, particularly a diabetes medication, without discussing it with your prescribing physician. Blood sugar management requires careful transition planning. Contact both your ophthalmologist and your prescribing endocrinologist or primary care physician together.
Step 6: Preserve All Records
From the moment you first seek care, your medical records become the foundation of any potential legal claim. Request copies of:
- Emergency room visit notes and discharge summary
- All ophthalmology examination records
- Lab results (ESR, CRP, blood glucose, HbA1c)
- Pharmacy records confirming your GLP-1 prescription and fill history
- Any imaging performed (OCT reports, fundus photographs, MRI if obtained)
Do not assume these records will be easy to obtain later. Request them now, keep copies in a safe place, and share them with a GLP-1 litigation attorney as soon as possible.
For a complete documentation guide, read: NAION Eye Tests Required for Vision Loss Claims: A Complete Guide
Causes of Sudden Vision Loss: A Quick Reference Guide
The following table summarizes the most common causes of sudden vision loss, their key distinguishing features, and urgency level:
| Condition | Pain? | Which Eye? | Key Features | Time-Critical? |
|---|---|---|---|---|
| NAION | None | One | Worse on waking; inferior field loss; hyperemic swollen disc; GLP-1 risk factor | Urgent — no reversal, but acute window for diagnosis & fellow-eye protection |
| AAION (GCA) | Sometimes headache | One (then both) | Jaw pain, scalp tenderness, ESR/CRP elevated; pale disc | True emergency: IV steroids immediately |
| CRAO (Eye Stroke) | None | One | Cherry-red spot; retinal pallor; carotid/cardiac source | Minutes matter; tPA/HBO within hours |
| Retinal Detachment | None | One | Floaters + flashes then curtain; spreading from periphery | Emergency surgery; macula-off: hours |
| Acute Angle-Closure Glaucoma | Severe | One | Halos, nausea, rock-hard eye, very high IOP | Emergency; pressure drops within hours |
| Amaurosis Fugax | None | One | Lasts minutes then resolves; curtain up and down | Stroke risk; ER immediately even if resolved |
| Optic Neuritis | With eye movement | One | Young patient; pain; MS history; MRI enhancement | Urgent, IV steroids speed recovery |
| Vitreous Hemorrhage | None | One | Sudden floaters / red haze / cobwebs; diabetic history | Urgent; may mask retinal tear/detachment |
| Stroke (cortical) | None | Both (same side) | Bilateral field cut; other stroke signs | Call 911; tPA within 4.5 hours |
| Migraine with Aura | Often | Both | Zigzag / scintillating scotoma; resolves in 20–60 min | Typically benign, but first episode needs evaluation |
For GLP-1 Users: Baseline Eye Exams Before and During Treatment
Because NAION can begin silently, and because identifying structural optic nerve risk factors before starting a GLP-1 drug may allow for closer monitoring, leading ophthalmology organizations now recommend:
Before Starting a GLP-1 Drug
- A comprehensive baseline eye examination including dilated fundus evaluation to assess optic disc size and cup-to-disc ratio, identifying a “disc at risk” (small cup with crowded nerve fibers) before treatment begins
- Documentation of any pre-existing optic nerve conditions, glaucoma, or vascular eye disease
- Discussion of NAION risk with the prescribing physician if you have multiple vascular risk factors (diabetes, hypertension, OSA, previous NAION in the fellow eye)
While Taking a GLP-1 Drug
- Annual comprehensive eye exams at minimum, more frequent if at higher risk
- Prompt evaluation of any new visual symptoms, do not wait for your annual exam
- The daily one-eye cover test described above as a simple morning self-check
- If you develop NAION in one eye, aggressive monitoring of the fellow eye at least every 6 months, given the 15–25% risk of fellow-eye involvement within five years
After a Vision Loss Event
- Emergency evaluation as described above
- Neuro-ophthalmology consultation within days
- Full NAION diagnostic workup including OCT and visual field testing
- Consideration of GLP-1 drug discontinuation in coordination with your prescribing physician, per EMA/WHO guidance
Q&A: Sudden Vision Loss and GLP-1 Drugs
Q1. I woke up this morning and one eye seems blurry. Should I go to the ER?
Yes. Call your ophthalmologist’s emergency line immediately or go to the emergency room. Sudden vision loss noticed upon waking is the classic presentation of NAION, but it can also indicate a retinal artery occlusion or other conditions that may be time-sensitive. Do not wait to see if it resolves. Tell the clinician you are on a GLP-1 drug.
Q2. My vision came back after about 10 minutes. Do I still need emergency care?
Yes, absolutely. Transient vision loss that resolves, known as amaurosis fugax, is a potential TIA (mini-stroke) and carries a 10–15% risk of full stroke within the first year if the underlying cause is not identified and treated. Vision returning to normal does not make the episode safe. Go to an emergency room the same day, even if you feel completely fine.
Q3. Can the emergency room diagnose NAION?
The ER can perform initial evaluation including dilated fundus examination, visual acuity, intraocular pressure, and blood tests for ESR/CRP. This is usually sufficient to identify NAION as the working diagnosis and rule out more immediately life-threatening conditions like stroke and GCA. However, a full NAION workup including formal visual field testing and OCT requires follow-up with an ophthalmologist or neuro-ophthalmologist within days of the acute event.
Q4. Should I stop my Ozempic or Wegovy immediately if I think I have NAION?
Do not stop your GLP-1 medication without medical guidance, especially if you have diabetes. Abruptly stopping a diabetes medication can cause dangerous blood sugar swings. Contact your prescribing physician immediately alongside seeking ophthalmology care; they can help you manage the transition safely. Once NAION is confirmed, the European Medicines Agency and WHO recommend discontinuing semaglutide, but this should be done under medical supervision with appropriate diabetes management in place.
Q5. How do I tell if my vision loss is NAION or a stroke?
Both can cause sudden vision loss, but they have important differences. NAION causes painless vision loss in one eye only, typically noticed upon waking, with loss of the top or bottom half of the visual field. Stroke affecting the visual system (occipital cortex) typically causes a visual field loss that affects the same side in both eyes simultaneously; you lose the right half of vision in both eyes, for example. Stroke also commonly has other signs: facial drooping, arm weakness, slurred speech, confusion. If any of these accompany vision loss, call 911 immediately for stroke response. When in doubt, treat it as a stroke emergency until proven otherwise.
Q6. Is NAION vision loss immediately obvious, or can it come on gradually?
NAION is characteristically sudden. The vision loss is typically present from the moment of waking or is noticed abruptly during waking hours. Unlike glaucoma (which progresses silently over years) or optic neuritis (which may worsen over days), NAION vision loss is maximal or near-maximal at onset. Some patients notice the loss more gradually over a day or two as edema evolves, but this is less typical. If vision loss is progressing steadily over weeks, NAION is less likely and other diagnoses (compressive lesion, optic neuritis) must be evaluated.
Q7. What should I tell the ER doctor if I’m on a GLP-1 drug?
Tell them immediately: the name and dose of your GLP-1 medication, how long you have been taking it, any recent dose changes, and that you are aware of a published connection between GLP-1 drugs and NAION. Ask them to document the GLP-1 use in relation to your vision loss in the medical record. Ask for an ophthalmology consult or urgent referral. Request copies of all records, including the optic disc exam findings, visual acuity measurements, and any blood test results.
You Are Not Alone: The GLP-1 NAION Legal Landscape
If you experienced sudden vision loss or were diagnosed with NAION while taking a GLP-1 drug, you may be one of a growing number of patients whose experiences have triggered the creation of MDL No. 3163, a new federal multidistrict litigation specifically for GLP-1 NAION vision loss claims, created in December 2025. Plaintiffs allege that manufacturers including Novo Nordisk (Ozempic, Wegovy) and Eli Lilly (Mounjaro, Zepbound) failed to adequately warn patients and prescribers about the risk of NAION and permanent optic nerve injury.
The European Medicines Agency and WHO have formally recognized NAION as a rare side effect of semaglutide and issued safety communications, but the FDA has not yet required a corresponding NAION warning on U.S. drug labels. This regulatory gap is central to the failure-to-warn litigation claims.
For the full litigation update including MDL status and what to expect, read: NAION MDL Update: GLP-1 Vision Loss Litigation Status
Why Work With Us
Exclusive Focus on GLP-1 Injuries
Our practice is dedicated entirely to GLP-1 medication injuries, including NAION vision loss, gastroparesis, ileus, and related complications. We are not generalists; this is our core focus.
- Deep familiarity with how NAION presents clinically, what records are needed, and how to build a strong case
- Current knowledge of MDL 3163, case management orders, Plaintiff Fact Sheet requirements, and litigation strategy
- Commitment to acting fast, because the statute of limitations on your claim is running from the date of your injury
Integrated Medical Expert Network
We work with board-certified ophthalmologists, neuro-ophthalmologists, pharmacologists, and life-care planners who understand NAION, both as a medical diagnosis and as the foundation of a legal damages claim.
No Upfront Costs
We represent all GLP-1 clients on a pure contingency-fee basis:
- No fees unless we win
- We advance all costs of experts, records, and litigation
- Free initial consultation: no obligation, no risk
Compassionate, Experienced Support
Sudden vision loss is terrifying. We understand that you are navigating a medical crisis and a legal decision simultaneously. We will guide you through both, clearly, promptly, and with genuine care for your outcome.
Contact Us for a Free Consultation
If you took a GLP-1 drug and experienced sudden vision loss — act on both fronts: medical and legal.
Visit www.GLP1Lawsuits.com to:
- Get a free case evaluation
- Speak with an experienced pharmaceutical-litigation attorney about your NAION vision loss
- Learn more about MDL 3163 and your legal options
- Get a timeline-specific analysis of your GLP-1 use, diagnosis, and documentation
- Join others seeking justice for preventable, permanent vision loss
The statute of limitations is running. Contact us today. No upfront fees and no costs unless we win your case.
Sources Cited
| # | Authority | Description |
|---|---|---|
| 1 | Cleveland Clinic - Sudden Vision Loss | “Sudden vision loss is a medical emergency. Call 911 or go to an emergency room immediately.” Clinical overview of causes and emergency response guidance |
| 2 | ClearView Eyes - Eye Emergencies: ER vs. Urgent Care | “More than 7 million Americans experience sudden vision loss annually”; ER vs. urgent care decision guide; time window for CRAO (February 2026) |
| 3 | PMC - CRAO Retinal Survival Time (PMC5907384) | Retinal infarction occurs after as little as 12–15 minutes of complete CRAO; 240-minute threshold for massive irreversible ischemia; treatment implications |
| 4 | Nature - CRAO: A Stroke of the Eye | “Time is critical in acute CRAO”; 240-minute cut-off; comparison to 4.5-hour stroke thrombolysis window; tPA and hyperbaric oxygen data (2024) |
| 5 | AHA Scientific Statement - Management of CRAO | Time-critical management of central retinal artery occlusion; stroke comorbidity; emergency workup protocol (2021) |
| 6 | Mayo Clinic / Cleveland Clinic - Giant Cell Arteritis | Emergency high-dose steroids must begin immediately before biopsy confirmation; IV methylprednisolone for active vision loss; fellow-eye protection rationale |
| 7 | Eyes on Eyecare - GCA Ophthalmic Emergency Series | Immediate steroid protocol: prednisone 1 mg/kg; methylprednisolone IV for vision loss; taper over 18–24 months; TAB gold standard |
| 8 | NIH StatPearls - Amaurosis Fugax (NBK470528) | Transient monocular vision loss as TIA equivalent; 10–15% stroke risk within 1 year if untreated; emergency evaluation required even after vision returns (2025) |
| 9 | Healthline / GoodRx - Amaurosis Fugax | “Think of it as a temporary stroke that affects the eye”; carotid artery source; stroke prevention rationale for emergency evaluation |
| 10 | Lake Norman Eye Care - GLP-1 and NAION | Specific guidance for GLP-1 users: symptoms prompting immediate evaluation, one-eye cover test, morning vision check, baseline exam recommendations (September 2025) |
| 11 | Today.com / NBC News - GLP-1 Drugs and Eyes | Expert guidance on monitoring vision on GLP-1 drugs; Dr. VanderBeek, Dr. Garg commentary on self-testing and prompt evaluation (August 2025) |
| 12 | WebMD - Ozempic Blindness | NAION emergency guidance: “If there’s something to be done, the time period is maybe within the first one or two hours”; risk factors; irreversibility (June 2025) |
| 13 | Geeky Medics - Sudden Painless Vision Loss | Differential diagnosis of acute painless vision loss; NAION vs. CRAO vs. retinal detachment vs. GCA clinical distinguishing features |
| 14 | Time of Care - Differential Diagnosis: Acute Painless Vision Loss | Complete differential including retinal artery/vein occlusion, detachment, macular degeneration, optic neuritis, NAION, GCA, vitreous hemorrhage |
| 15 | NIH StatPearls - NAION (NBK559045) | NAION pathophysiology: nocturnal hypotension, compartment syndrome cascade, morning-onset pattern; systemic risk factors (September 2025) |
| 16 | American Optometric Association (AOA) | Baseline and monitoring eye exam guidance for GLP-1 users; disc-at-risk evaluation; NAION risk counseling |
| 17 | JPML Transfer Order - MDL No. 3163 | New NAION MDL creation; December 2025 |
| 18 | EMA / WHO | Formal NAION classification as very rare semaglutide side effect; discontinuation recommendation for confirmed NAION; June 2025 |
Disclaimer
This article provides general medical and legal information about sudden vision loss, NAION, and GLP-1 litigation and does not constitute medical or legal advice. If you are experiencing vision loss right now, stop reading and seek emergency medical care immediately. For diagnosis, treatment, and medication decisions, consult a qualified healthcare provider — including an ophthalmologist, neuro-ophthalmologist, or emergency medicine physician. For guidance on your legal rights and options, consult a licensed pharmaceutical litigation attorney. Each case is unique; past results do not guarantee future outcomes.
© 2026 GLP1lawsuits.com | All Rights Reserved
Last reviewed by a licensed attorney: March 2026